 CONTACT
CONTACT





- ERNs
- Patient Stories
- CAROLINE'S STORY
CAROLINE’S STORY
- February 26th, 2026
- VASCERN. ERN on multisystemic vascular diseases
-
 Netherlands
Netherlands
- Share
The patient journey of Tristan, born with an infantile hemangioma XL
Meet Tristan, my middle son, born at term when I was 35 years old. Shortly after birth, the midwife realised that he needed to be seen by an academic centre specialising in vascular anomalies. Tristan was therefore referred to the academic hospital in Amsterdam with an unusually large segmental infantile hemangioma (IH).
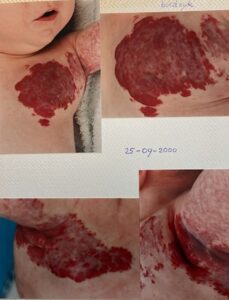
Due to the very large size and rapid growth of the hemangioma, ulcerations developed, which often caused severe bleeding. Tristan developed a so-called “sports heart”: his left ventricle enlarged to 150% of normal size, and he required heart medication. Because of the frequent bleeding episodes, his haemoglobin levels often dropped dangerously low, leading to repeated hospitalisations for blood transfusions.
For two years, infections from both ears circulated back and forth to the hemangioma wounds. During this time, he received litres of antibiotics and countless types of ointments to try to control the infections. Because of the volume of the hemangioma, Tristan’s body did not grow straight but became asymmetrical, and he therefore received physiotherapy.
One night, just before going to bed, we found him covered in blood. My husband packed his blood-soaked clothes and bedding in a garbage bag as we raced to the emergency room to show the seriousness of the situation. The ER doctors reacted quickly and managed to place an IV line—something that was by then extremely difficult. It was estimated that Tristan had lost a significant amount of blood.
Because I worked internationally, we had to hire a private nurse to assist my husband with wound care and dressing changes, using surgical sponges (Spongostan) to control arterial bleeding when it occurred.

The wounds became completely destabilised due to the many medications and ointments—a vicious circle. All types of wound dressings were tried, including silicone dressings, but they all adhered to the wounds. As a result, dressing changes could only be done after soaking him in the bath.

As an experiment, the Burn Centre in Beverwijk applied Honeysoft dressings to Tristan, which had previously been tested on pigs with burn wounds. During one check-up, a male nurse specialised in burn wounds thought he could help by removing the dressings himself. On burn wounds, honey gauze does not stick, but the wound beds of Tristan’s hemangioma were extremely unstable. I had explained the necessity of soaking the dressings in warm water beforehand. Nevertheless, the nurse pulled on them, causing immediate bleeding. Panic followed.
In short: my advice to doctors is to listen to caregivers who deal with children with special needs on a daily basis.
After two years of constant hospital visits, being stared at on beaches and playgrounds, and witnessing the trauma of IV placements for blood transfusions (sometimes requiring attempts in all hands and feet while he cried inconsolably), the situation took a serious toll on my mental stability.
However, as infantile hemangiomas eventually regress, Tristan slowly improved.
After all the bandages, wounds, and blood disappeared, you can now see the final result: a fine young man – just a little afraid of needles.

A few years after the crisis period, together with another mother, we founded HEVAS in 2007, the patient organisation for vascular anomalies (vascular tumours such as IH and vascular malformations) in the Netherlands. Through HEVAS, we help parents and patients find the appropriate centres of expertise and specialised doctors, and we provide peer support. We also organise conferences on vascular anomalies for non-specialized doctors and child health clinic doctors, in cooperation with our National Network of Centres of Expertise.
In addition, I have been active as an ePAG representative in VASCERN since the start of the European Reference Networks in 2017 in Vilnius. Together with 7 fellow European patient advocates, we share the latest knowledge with patient organisations across Europe. Within VASCERN, we work in close partnership with specialised physicians in vascular anomalies, bringing the patient perspective to the table.
My latest challenge is the formation of a Patient Support Committee within ISSVA (the International Society for the Study of Vascular Anomalies), together with an American colleague, planned for 2026. In this role, I hope to continue being of value to patients with vascular anomalies and to promote VASCERN as a powerful European example of cross-border collaboration between specialists, improving care and treatment for people living with rare diseases.




